Talk:Clonazepam
| Pharmacology Start‑class Mid‑importance | ||||||||||
| ||||||||||

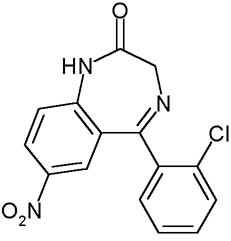
The image of the chemical structure of Clonazepam was taken from http://www.biopsychiatry.com/clonazepam/clonazepam.jpg
{kind=link}
I e-mailed the owner of biopsychiatry.com at info@bltc.com and asked permission to use his images and content on Wikipedia.
He replied thus:
David Pearce wrote:
> At 20:03 08/06/2004, you wrote:
>
>> What is your policy on allowing images and text from your HedWeb site to be used on Wikipedia?
>
> Hi Mike
> You're welcome to use anything of interest
> The Wikipedia is a fantastic project!
> very best wishes from sunny Brighton
> Dave
Pardon the intrusion. However I am a college student in New York studying chemistry and pharmacology and was wondering if anyone could inform me as to what mechanism of action tobacco's role plays in decreasing the effects of Clonezapam (Klonopin), and Diazepam (Valium). Username: a1970sweet If anyone has any information regarding this matter I would greatly appreciate it and if you could simply post it under my paragraph here. Thank-you.
Safe taking with Sleep Apnea?
Is Clonazepam meant to be taken in the morning after breakfast and/or as a sleep/anxiety aid just before bedtime?
Response: I don't know if it is safe with sleep apnea, but regarding when it is meant to be taken...it depends upon the specific situation of the patient and judgment of the prescribing physician. Anxiety sufferers may take Clonazepam at any time during the day as an "as needed" medication or as a maintenance treatment. For others, it is used as a sleep aid. For example, some anti-depressants are engergizing (Effexor for example) which make it difficult for those taking it to sleep. Low doses of Clonazepam may be prescribed in that situation to be taken in the evening. Tobycat 03:36, 20 Apr 2005 (UTC)
I was diagnosed as a Textbook "REM Sleep disorder", In which I talk, move, and walk during sleep. My Sleep clinic doctor prescribed me 5mg Clonazepam before bedtime, then doubled the dose to 10mg when that didn't do anything for me. Qexter 08:36, 8 Jun 2006 (EST)
5 mg of clonazepam is a huge dose to take all at once; 10 mg - taken as a single dose - is practically an anesthetic. Either you were taking DIazepam (Valium), for which these would be normal doses, or you left out a couple of decimal points. Did you mean 0.5 mg and 1.0 mg, Qexter? If not, and you really were taking these high doses of Klono, you must have been very sleepy the next day. 68.83.140.156 04:56, 24 August 2006 (UTC)Essex9999
I have obstructive sleep apnea (for 16 years now with CPAP) and have been taking 2 mg of Clonazepam about 1 hr before I want to pass out. I awake either six hours later if my bladder is full and go back for my REM sleep (which for me is after six hours of sleep usualy) or usually sleep eight to nine hours. I feel great when I wake up.
What is the dose of Clonazepam conpared to Valium and Xanax?
What is normal dose for medical, and recreational use of clonazepam?
- Recreational use of clonazapam? Go away. JFW | T@lk 07:50, 17 July 2005 (UTC)
- That was a very rude comment from someone who indulges in the recreational use of drugs such as alcohol and coffee, according to his user page. Stanfordandson 01:07, 22 June 2006 (UTC)
- Hey, this is useful (potentially life-saving) information (recreational doses are generally well within the range of medicinal doses). In general:
- Diazepam (Valium) 10mg
- Alprazolam (Xanax) 0.5mg
- Clonazepam (Klonopin) 0.5mg
- Lorazepam (Ativan) 1.0mg
- Temazepam (Restoril) 20mg
- A starter dose is typically somewhat below that benchmark (0.5mg Ativan, for example) but the above are all generally equivalent and is a usual dose for a benzodiazepine. The dose builds with tolerance (I know somebody who takes 4mg Klonopin daily for maintenance, which comes out to dosing (in theory) eight times a day). Benzos aren't very fun in general unless you need them and can be very nasty indeed. A word to the wise.
Heart beats and Clonazepam
A daily, small dose of Clonazepam (0.5mg or less) can cause high heart beats? Like 130-150 in a "normal" state, not doing exercise or heavy physical activity.
Response: seems unlikely. I was having some mild panic attacks, with symptoms including a racing heart, and was prescribed low dose Clonazepam for as-needed treatment.
Indication vs. Approval
Regarding Davidruben's revert to the indications section (http://en.wikipedia.org/w/index.php?title=Clonazepam&diff=prev&oldid=74429734): Look at the sentence on Tourette Syndrome. It's clearly confusing FDA approval with the more general concept of a commonly-accepted use. And what's the point of even mentioning that something is an off-label use (which is, after all, a US-specific regulatory issue) in a general article on the substance? I can see it in the case of Vioxx, but not here. KonradG 00:53, 8 September 2006 (UTC)
- I agree in part. "Off-label" use probably exceeds FDA approved use for many drugs, even if we limit our discussion to the United States. Even before FDA approval as an anxiolytic in the late 90s, Klonopin was far more often prescribed for anxiety than the relatively few and exotic convulsive disorders for which it was officially approved in 1975. Having said that, simply denoting which indications are FDA sanctioned is useful for a potential consumer. Many off label uses rely exclusively on anecdotal evidence JE1977 02:30, 4 March 2007 (UTC)
- I find that's very rarely the case. Can you name a single example? A drug's indication represents the mainstream view of the medical community. Any claim that a particular indication is not backed by evidence is therefore not a mainstream view, and as such needs to have solid references. The fact that a particular use is off-label doesn't tell you anything by itself. And in almost all cases will mislead the average consumer because "approval" is such a vague word. KonradG 03:54, 6 March 2007 (UTC)
- Indications for a particular drug vary by which text one consults. My fault, when I say anecdotal evidence I mean clinical experience (i.e. no scientific studies exist or only low quality studies exist to recommend a drug for a particular purpose) Case in point: the practice of prescribing Dexedrine to augment Nardil. Conventional wisdom says this is huge no no, but experienced psychiatrists do just this albeit with strict blood pressure monitoring. Prescribing opiates as a last ditch attempt to alleviate treatment resistant severe depression is another. Many doctors will not deviate from the indications on the label for fear of legal liability (especially true concerning scheduled drugs) and some insurance companies will not pay for "off label" prescriptions. So it is useful for consumers to know the FDA labeled indications. Plus listing the FDA labeled indications is standard on pretty much all drug monographs printed in America. JE1977 02:46, 7 March 2007 (UTC)
- Monographs contain that info because they're legally required to. Encyclopedias aren't, and therefore they're free to get medical information from doctors instead of lawyers. Anyway, what you're talking about are experimental treatments, not indications. There's no reason to mention that an indication is off-label, especially when you don't even know if the reader is from the US. As for a doctor's legal liability, that isn't affected by FDA approval, except as far as it provides evidence that the use was a medically accepted one. The FDA doesn't regulate medical practice. KonradG 17:16, 7 March 2007 (UTC)
Clonazepam Hangover
I am a long-term user of Clonazepam for generalized anxiety disorder since I was 17 and I and others who have taken my medication have noticed a distinct "Clonazepam Hangover" effect. When you take it before you go to bed, you wake up feeling many similar symptoms of an alcohol hangover such as dizziness, irritability, drowsiness, and a headache. This is probably due to the half-life of the medication in your system as well as the way it interacts with your brain while you sleep, as benzos in general have a tendency to interfere with REM sleep. If you don't mind I would like to add a small segment containing some information about such, as I am a long-term user. I will not couch it in absolute language but instead say "Some users complain of "hangover like" symptoms." or something like that. —The preceding unsigned comment was added by Bbcrackmonkey (talk • contribs) 12:02, 13 February 2007 (UTC).
- Go for it, but make sure it's verifiable from somewhere other than your own experience. That generally means the information has to have been published somewhere in a reliable source. KonradG 12:16, 13 February 2007 (UTC)
It appears that the publicists at Roche Pharmacy keep editing this entry to downplay clonazepam's negative effects. We'll see what tune they sing when the class-action lawsuit against mis-prescribing of long-term clonazepam rolls around. There is no scientific evidence that benzodiazapines effectiviely treat insomnia or anxiety long-term. Shades of Upjohn, anyone? — Preceding unsigned comment added by 204.14.61.157 (talk • contribs) 21:53, 5 July 2007 (UTC) (comment moved from body of article by Precious Roy 11:36, 6 July 2007 (UTC))
- I have never worked for a pharmaceutical company, although I have been involved in pharmacological research, especially in expert systems for prescribing (i.e., I'm not a doctor but I play one on computers), and worked with medical school psychopharmacologists. Expert system rule bases do contain off-label indications, with appropriate cautions. Over the last few days, I have deleted anonymous opinions on clonazepam, which are in the form of attacks (as the above talk comment moved from the article page, accusing Roche publicists and making dark threats about class action).
- My concern is the apparent non-neutral point of view posts and edits regarding the long-term use of benzodiazepines in the range of anxiety disorders, including panic and social anxiety disorder. The short-term role of benzodiazepines is clear in these areas, but there are fewer studies of long-term effects: http://www.medscape.com/viewprogram/2997_pnt "Highlights of the International Congress of Biological Psychiatry [2004], Treatment of Anxiety Disorders: An Update", Pollock R and Kuo K.
- I do not argue that the core drugs for long-term treatment of panic disorder, social anxiety disorder, and generalized anxiety disorder are SSRIs (especially atypical ones) and anticonvulsants, as well as desensitization therapies such as CBT and EMDR. Benzodiazepines have a fairly clear short-term role. I see the issue as the role of benzodiazepines, especially clonazepam, in long-term treatment of patients resistant to the core drugs. From the Medscape survey, where the review authors cite Fisher PL, Durham RC. Psychol Med. 1999 Nov;29(6):1425-34 "Recovery rates in generalized anxiety disorder following psychological therapy: an analysis of clinically significant change in the STAI-T across outcome studies since 1990."
- From the cited review, "Fisher and Durham[64] conducted a reanalysis of 6 randomized, controlled trials of psychological therapy with GAD. Individual CBT and applied relaxation, focusing on excessive worry and physiological arousal, performed well, with overall recovery rates of 50% to 60% at 6-month follow-up. In general, GAD patients are responsive to treatment; however, they are also sensitive to medication side effects. Combined pharmacotherapy (eg, benzodiazepines plus SSRIs) or pharmacotherapy plus CBT may be appropriate for treatment-resistant patients" I see combined therapy as a legitimate off-label use in carefully selected patients.
- I suggest that this article be locked against anonymous updates. Howard C. Berkowitz 13:29, 6 July 2007 (UTC)